In June 2011, bpacnz produced a report on oxycodone dispensing which urged prescribers to review their use of oxycodone. Oxycodone is a strong opioid analgesic that should only be used as a second-line treatment for patients who are not able to tolerate morphine.
In this report 
View
/ Download pdf version of this report
In June 2011, bpacnz produced a report on oxycodone dispensing which urged prescribers to review their use
of oxycodone. Oxycodone is a strong opioid analgesic that should only be used as a second-line treatment for patients
who are not able to tolerate morphine.
This report will illustrate the following aspects of oxycodone dispensing in New Zealand:
- The number of people on oxycodone is still increasing
- While most patients are initiated on oxycodone outside general practice, a significant proportion of patients are
being started on oxycodone by general practitioners
- The length of treatment with oxycodone may be inappropriate for many patients
 For correspondence regarding oxycodone in NZ, see "Correspondence: Oxycodone and drivers of use", BPJ 45 (August, 2012).
For correspondence regarding oxycodone in NZ, see "Correspondence: Oxycodone and drivers of use", BPJ 45 (August, 2012).
National Trends
| 1 |
Oxycodone dispensing is still increasing
In the last five years (2007–11), the number of patients dispensed oxycodone increased 249%, while the number dispensed
morphine increased by only 18% (Figure 1). Overall, the number of patients dispensed an opioid is increasing each year
(78% over five years, compared to 4% population growth.
Oxycodone does not provide more effective pain relief than morphine, is more expensive, and is associated with increasing
levels of misuse. Therefore it should only be used in patients who do not tolerate morphine. |
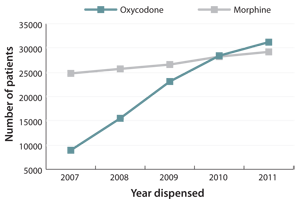
Figure 1: Number of patients dispensed oxycodone and morphine for years 2007–11 |
| 2 |
Oxycodone is frequently prescribed in general practice
In 2011, 22425 patients received their first oxycodone dispensing (no dispensing in the previous 12 months). The
majority of oxycodone was initiated outside general practice* but a significant proportion of patients were
either initiated (30%) or continued (17%) in general practice (Figure 2). |
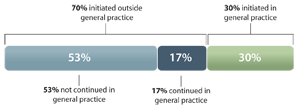
Figure 2: Source of oxycodone prescriptions for patients initiated in 2011 |
| 3 |
The length of oxycodone treatment may be inappropriate for many patients
Many patients may be treated with oxycodone for longer than is recommended. In 2011, 39% of patients were treated
continuously** for more than four weeks (Figure 3).
Long-term treatment with opioids is associated with adverse affects such as addiction, tolerance and increased sensitivity
to pain.1 Prescribers must be aware of the potential for misuse and addiction problems with oxycodone developing
in the community. |
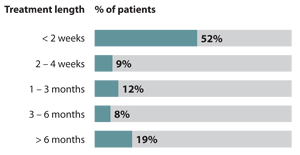
Figure 3: Proportion of patients by length of continuous treatment with oxycodone (2011) |
Notes and References
- • The data in this report includes all dispensings of morphine and oxycodone (excluding injectable formulations).
- * A GP was defined by membership in the bpacnz provider list of 4141 New Zealand general practitioners,
other prescribers are doctors working outside primary care.
- ** Continuous treatment with oxycodone was defined as a series of dispensings with no gaps greater than one month
between them.
- Manchikanti L, Fellows B, Ailinani H, Pampati V. Therapeutic use, abuse, and nonmedical use of opioids: a ten-year
perspective. Pain Physician 2010;13:401-35.