View / Download pdf version of this report
It is estimated that approximately 257,000 people have diagnosed diabetes in New Zealand.1 An annual diabetes review allows for assessment of glycaemic
control and earlier detection of, and intervention for, diabetes related complications. It also creates an opportunity to regularly review and assess individual
treatment plans and enable support if required. Additionally, the information gained from diabetes follow-up provides up to date data for diabetes
registers, which in turn drives improvements in diabetes service delivery.2
Each DHB is responsible for their own diabetes care improvement package, which is a community and
primary care-based programme and therefore services and initiatives differ between regions.
Regular checks for the management of diabetes
The New Zealand quality standards for diabetes care state that: "People with diabetes should be offered, as a
minimum, an annual assessment for the risk and presence of diabetes-related complications and for cardiovascular
risk. They should participate in making their own care plans, and set agreed and documented goals/targets with their
health care team." 3
The table below suggests the assessments that should be conducted at least annually. The frequency of these
may vary depending on the individual patient’s risk of complications.2,5
|
Assess at least Annually |
If moderate to high risk of complications |
| HbA1c |
 |
3 monthly |
| Blood Pressure |
at every visit |
|
| Lipid profile |
|
|
| Feet |
|
3 monthly |
| Retina check |
|
|
| Albumin / Creatinine ratio |
|
6 monthly |
| eGFR |
|
|
| BMI / Weight |
|
|
| Teeth and gums |
|
|
| Healthy lifestyle advice |
|
|
Increasing uptake of the annual diabetes review 4
Strategies to increase the number of people with diabetes who receive annual follow-ups include:
- Send out a recall letter or create an electronic alert: Recall alerts can be created for patients overdue for an annual
assessment
- Create a diabetes register: An electronic diabetes register allows analysis of a practice’s population, which can
highlight patients who are overdue for review and those not achieving treatment targets
- Elect a chronic conditions “champion”: Allocate specific roles for members of the primary care team to oversee aspects
of the diabetes programme and patient recall
- Promote patient awareness: High visibility posters, leaflets and advertising in the practice may encourage patients
to attend annual assessments
- Text alert reminders: Text alerts are a simple, cheap and non-intrusive way to remind patients when their annual assessments
are due
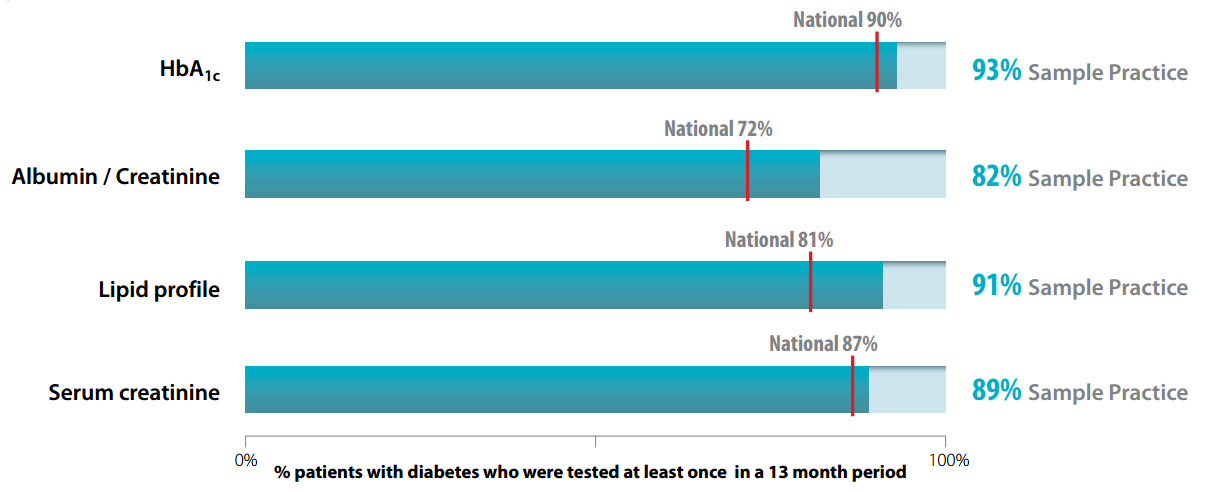
Monitoring
The results below show whether tests of HbA1c, microalbumin (to calculate an albumin/creatinine ratio), serum
creatinine (to calculate eGRF) and serum cholesterol (lipid profile) are being requested at least annually for
patients with diabetes, both nationally and at your practice. The data in this report is for all registered patients
dispensed either insulin, oral diabetes medicine or testing strips between March, 2014 and March, 2015.
Sample Practice
- Ministry of Health (MOH). Virtual Diabetes Register. MOH, 2014. Available from:
www.health.govt.nz (Accessed July, 2015).
- New Zealand Guidelines Group. New Zealand Primary Care Handbook, 2012. Available from:
www.health.govt.nz (Accessed July, 2015).
- Ministry of Health. Quality Standards for Diabetes Care Toolkit. Wellington: Ministry of Health, 2014.
- bpacnz. Diabetes follow-up. Best Practice Journal 2011; 39. Available from:
www.bpac.org.nz (Accessed July, 2015).
- Health Mentor Online. Diabetes resources for healthcare professionals. Available from:
www.pro.healthmentoronline.com (Accessed July, 2015)